
-(1).png)
-(1).png)

Contributed equally as first authors
Simulation-based education (SBE) is increasingly recognised as a key innovation in clinical training and patient safety, particularly in low- and middle-income countries (LMICs). However, the scale and diffusion of SBE in Pakistan remain unclear. This systematic review maps the national adoption using Rogers’ Diffusion of Innovation (DOI) framework.
A PRISMA-guided systematic review registered in PROSPERO searched PubMed, CINAHL, PsycINFO and PakMediNet through 22 July 2025 (final search date) for English- and non-English studies reporting original SBE interventions in medical training in Pakistan. Dual independent screening, data extraction and risk-of-bias assessment were performed using validated tools. Key data (study design, professional group, modality, DOI stage, Kirkpatrick level, barriers/facilitators) were extracted and summarised descriptively.
Seventy-three studies met the inclusion criteria across multiple specialties and simulation modalities. Most interventions were at the Persuasion (41/73, 56%) or Knowledge (19/73, 26%) stages of DOI and were delivered as short-term workshops, with outcomes primarily limited to participant satisfaction and knowledge or skills acquisition (Kirkpatrick levels 1–2). Only six studies reached the Decision stage and three reported Implementation or Confirmation (structured integration or sustained use). Reported barriers included infrastructure limitations (65%), faculty shortages and lack of funding, while facilitators included local innovation, faculty development and institutional collaboration. No studies reported patient- or system-level outcomes.
SBE in Pakistan shows isolated innovation but slow diffusion, with gaps in curriculum integration and higher-level evaluation. Barriers mirror those reported across LMICs in South and Southeast Asia. Advancing scalable implementation will require national policy support, funding investment, accredited faculty development and structured evaluation. These findings provide an opportunity map to integrate SBE in medical education systematically.
What this study adds
•This is the first PROSPERO-registered national systematic review of simulation-based education (SBE) in Pakistan, using PRISMA-guided methods and librarian-supported multi-database searching, including a national database.
•It focuses specifically on implemented SBE interventions and integrates Rogers’ Diffusion of Innovation (DOI) framework with the Kirkpatrick evaluation model to provide a structured national mapping of adoption and evaluation maturity.
•Using standardised, design-specific risk-of-bias tools (JBI and NIH), each study was categorised by DOI stage and corresponding Kirkpatrick outcome level, enabling a theory-informed analysis of implementation progression.
•The review demonstrates that most SBE initiatives remain at early diffusion stages, with evaluation largely limited to learner satisfaction and knowledge outcomes and with no reported patient- or system-level impact.
•This study establishes a national baseline evidence map to inform policy, faculty development, funding priorities and scalable integration strategies for advancing SBE in Pakistan and comparable LMIC settings.
With the advancement of technology, simulation has emerged as a revolutionary means of training, initially used in aviation and military fields before rapidly gaining traction in healthcare education [1]. The growing adoption of simulation in medical training is mainly due to its capacity to provide a controlled environment for skill development without compromising patient care [2]. While high-income countries have made significant progress in implementing simulation-based education (SBE), low- and middle-income countries (LMICs) and nations with limited resources, including Pakistan, have relatively recently begun this integration [3,4].
Pakistan, with a large and growing population of around 242 million and a constrained physician workforce of approximately 1.1 doctors per 1000 people, faces substantial pressure on its health system [3]. Medical education in Pakistan is governed by a national regulatory framework led by the Pakistan Medical and Dental Council (PMDC) under federal law, in coordination with the Higher Education Commission (HEC) and provincial authorities [5,6]. Admissions are regulated through the Medical and Dental College Admission Test (MDCAT), organised by the PMDC and designated universities [7].
The medical education model continues to rely heavily on the traditional ‘see one, do one, teach one’ approach, an opportunistic model that can slow learning, result in inconsistent exposure to critical skills and pose risks to patient safety [3]. These challenges have been amplified by sociocultural constraints and crises such as the COVID‑19 pandemic [4]. In this context, simulation‑based education (SBE) offers a reliable and ethical alternative, allowing learners to acquire essential clinical skills in a controlled, risk‑free environment while safeguarding patient welfare [2].
Simulation‑based education is recognised for its potential to improve healthcare quality and safety by providing scalable, efficient and standardised training. Despite this promise, the adoption and integration of SBE across medical education in Pakistan remain fragmented, mirroring patterns reported in other LMICs where infrastructure, funding and faculty capacity limit diffusion beyond early adopters [2,3]. Beyond these disparities, there is an overarching gap: the current situation and scope of intervention‑based SBE in Pakistan have not been synthesised with attention to study quality, adoption stage or outcome level, which hinders strategic progress.
Prior to this systematic review, we conducted a comprehensive scoping review of healthcare simulation in Pakistan that mapped study types, professions and simulation modalities [3]. While that review provided a broad landscape analysis, it did not evaluate intervention quality or adoption processes. Building on these findings, the present systematic review focuses specifically on SBE interventions in medical training using Rogers’ Diffusion of Innovation (DOI) framework [8–10].
This study is grounded in (1) the DOI theory, which provides a structured framework for understanding how new practices spread through professional communities and (2) Kirkpatrick’s model of training evaluation [11], which categorises outcomes from learner reactions to system‑level impacts [8–10]. By applying these frameworks, the review examines where Pakistani SBE initiatives sit within the DOI stages (knowledge, persuasion, decision, implementation, confirmation), which outcome levels are being achieved and where improvement is warranted.
This PROSPERO-registered systematic review is the first to synthesise SBE evidence in Pakistan’s medical education system using structured risk-of-bias assessment, ensuring rigour and transferability to similar LMIC settings. The goal of this systematic review is to describe the adoption, barriers, enablers and future directions for SBE within the DOI theory framework. The objectives are to: (1) describe the current state of intervention‑based medical SBE in Pakistan through the lens of DOI, (2) identify barriers and enablers influencing diffusion and integration and (3) outline future directions for strengthening SBE design, scale‑up and evaluation in Pakistan and comparable lower‑middle‑income contexts.
This systematic review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines and the registered protocol (CRD42023453962) [12,13] (Figure 1).

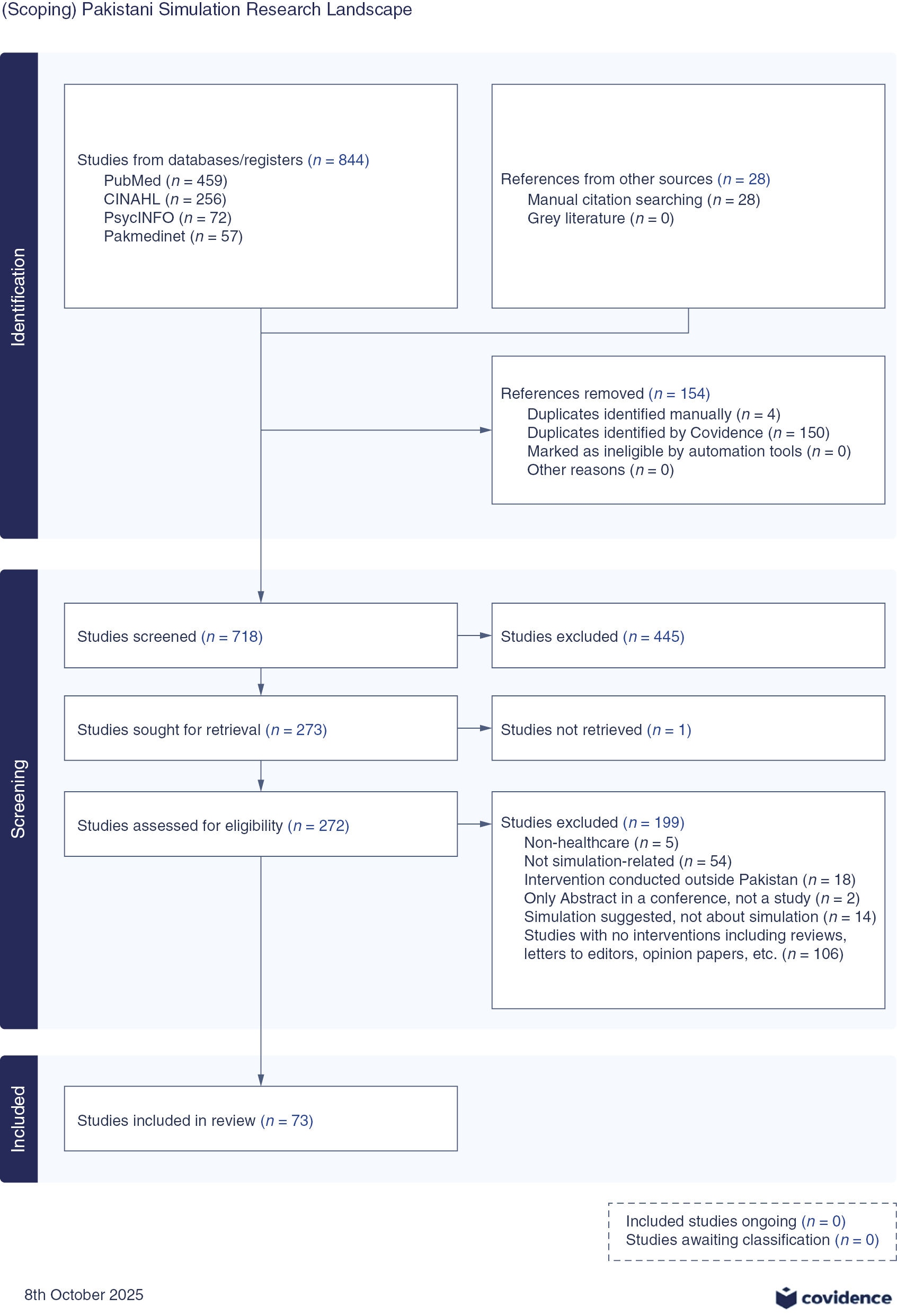
PRISMA flow diagram
We included studies on simulation-based interventions in medical education and training in Pakistan, with no language restrictions. Eligible studies: (1) reported implemented SBE interventions in the medical field with any level of learners (undergraduate, postgraduate or continuing professional development) and (2) were conducted within the Pakistani healthcare or educational system, with at least one Pakistan-based author. We excluded studies unrelated to simulation, not focused on medical training, conducted outside Pakistan or involving mixed-country participants without disaggregated Pakistani data. Studies without Pakistani-based authors, even if published locally, were excluded. Reviews, editorials, letters, short communications, opinion pieces, conference abstracts and studies that only proposed or advocated simulation without implementation were also excluded.
We conducted a series of electronic searches, guided by a medical librarian from a leading healthcare institute, to identify eligible studies. Searches were performed on 25 September 2023, 29 February 2024, 3 July 2025 and 22 July 2025 across PubMed, CINAHL, PsycINFO and PakMediNet [14]. PakMediNet, a Pakistani database, was searched to broaden coverage because many Pakistani authors publish in regional journals that are not indexed in major international databases.
The tailored search strategy for each database comprised three components: (1) simulation terms, (2) education/training terms and (3) Pakistan terms, combined using Boolean operators. Controlled vocabulary (e.g. MeSH and CINAHL Headings) and free-text terms were used where applicable. In PakMediNet, which does not support complex Boolean queries, we manually searched combinations of simulation and education terms derived from the main strategies. Full search strategies for all databases are provided in Supplementary Material Appendix A. In addition, we manually searched the reference lists of all included studies to identify further eligible articles.
Citations from literature searches and reference list checks were imported into Covidence, where duplicates were removed [15]. To establish inter-rater reliability, three researchers (FN, NF, MB) independently screened the titles and abstracts of the first five studies and resolved inconsistencies through discussion. Subsequently, two reviewers independently screened all remaining titles and abstracts, with MB resolving disagreements through discussion and consensus.
For full-text screening, inter‑rater reliability was again established on five studies, followed by independent full‑text screening by two reviewers, with MB mediating any disagreements to reach consensus on inclusion or exclusion. Reasons for exclusion were documented during full-text screening. The overall study selection process is summarised in the PRISMA flow diagram (Figure 1).
For data collection, a data extraction sheet was developed in Covidence, pilot-tested on five randomly selected included articles, and then refined. For establishing the inter-rater reliability, all researchers independently extracted data for five studies, with conflicts resolved through discussion. Remaining data extraction was done independently by two researchers, with MB resolving conflicts. Cohen’s kappa (κ = 0.741) for inter-rater agreement was determined by Covidence [15], demonstrating strong agreement on the data points gathered by the researcher team. While this value is generally considered substantial agreement, it may suggest non-trivial disagreements regarding study design and outcomes. However, Covidence registers variations in data formatting (e.g. capitalisation differences, comma placement etc.) as discrepancies, which have marginally influenced the kappa value.
Extracted variables included: publication year, author details, study aim, study design, profession and learner level, simulation modality and description of the simulation activity, evaluation or assessment tools, tools’ psychometric properties (where reported) and simulation-relevant barriers and facilitating factors. Outcomes of each study were categorised using Kirkpatrick’s model as level 1 (reaction/satisfaction), level 2 (learning/knowledge/skills), level 3 (behaviour/change in practice) or level 4 (results/system impact) [11].
Because of high variability in study designs, participants and outcomes, conducting a meta-analysis was not possible. Given that this review aimed to understand the nature and scope of simulation-based interventions in Pakistan rather than calculate pooled effects, we conducted descriptive statistics (frequencies and proportions) to summarise key features of the studies. We synthesised the knowledge about the study foci through thematic analysis, and each study was also subsequently examined using the DOI framework to map the current landscape of simulation and identify strategies to improve adoption and scalability.
The thematic analysis of the primary foci was conducted by one author (FN) using Braun and Clarke’s framework [16], and was verified by another author (MB), with discrepancies resolved through discussion and review of the original study. Outcomes were mapped to Kirkpatrick levels (L1–L4) during data extraction. Using the combination of study foci and Kirkpatrick outcome levels, two authors (MB, FN) then independently assigned each study to one of Rogers’ five DOI stages using the following criteria:
1.Knowledge (Stage 1): initial introduction or report of simulation with no documented adoption evidence.
2.Persuasion (Stage 2): evaluation or testing of simulation effectiveness with awareness-building but no sustained practice documented.
3.Decision (Stage 3): evidence of adoption decision or follow-up data showing practitioners/faculty began using the intervention.
4.Implementation (Stage 4): regular curriculum integration with sustained institutional delivery.
5.Confirmation (Stage 5): multi-year routine use with documented continuation and community/system-level embedding.
Disagreements were resolved through discussion and re-review of original studies, with MB mediating final decisions. When available, we used follow-up data or longitudinal documentation of sustained use (e.g. multi-year ongoing delivery, faculty adoption post-training) to inform DOI stage assignment. Therefore, DOI stage assignment prioritised evidence of adoption and sustainability. Studies reporting lower Kirkpatrick levels (L1–L2) but with documented sustained use or follow-up showing adoption were classified at higher DOI stages (Implementation/Confirmation). See Figure 2.

Step-wise allocation of studies to DOI theory stages
We assessed risk of bias using the Joanna Briggs Institute (JBI) critical appraisal tools [17] for cross-sectional studies, case reports, quasi-experimental studies and RCTs and the National Heart, Lung and Blood Institute (NHLBI) tools [18] for pre-post studies without control groups. Two reviewers (MB, FN) independently applied the tools, recording supporting information and justifications for each domain. Discrepancies were resolved through discussion, and full item‑level ratings and thresholds are shown in Supplementary Material Appendix B.
The results are presented under three sections: (1) Study characteristics and simulation-specific details; (2) Simulation adoption using the DOI framework through analysis of studies’ focus and outcomes; (3) barriers, facilitators and contextual factors influencing simulation adoption are examined through the DOI lens.
Across 73 included studies [19–91] (see Supplementary Material Appendix C for study aims and RoB), the majority were published within the past decade, reflecting increased institutional attention to simulation in undergraduate and postgraduate medical education. Sixteen studies reported international collaboration, and such studies frequently described structured implementation strategies (n = 30) [24,32,70] and two demonstrated lower or medium RoB ratings [26,91]. Only six studies reported funding, while most did not disclose funding details and no clear association was observed between funding and RoB.
Studies primarily involved postgraduate trainees (n = 36) and undergraduate medical students (n = 27), with fewer interdisciplinary cohorts (n = 7), most frequently in emergency medicine, surgery, obstetrics and gynaecology, and critical care, fields commonly associated with high-acuity or procedural simulation (Figure 3).
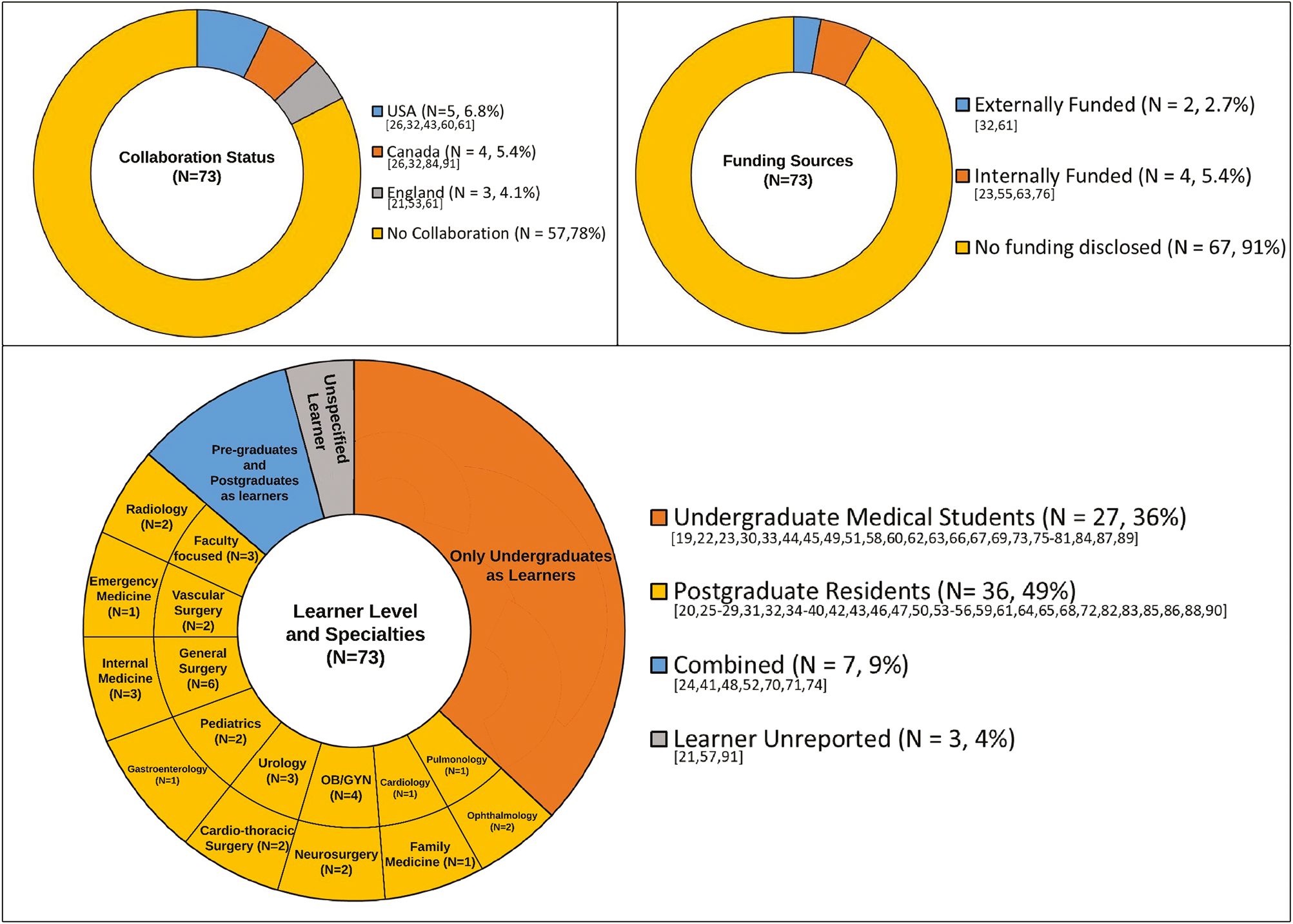
Collaboration status, funding sources and learner characteristics across included studies (N = 73)
Simulation sessions varied in structure and instructional depth. Table 1 summarises studies with structured simulation activities and assessment. Key instructional components, including pre-learning materials, debriefing and small-group discussions, were inconsistently reported. Only a subset described trained simulation facilitators. Evaluation outcomes focused mainly on learner satisfaction and knowledge gain, with fewer studies assessing behavioural outcomes or system-level impact.

| Description of sessions | Studies count (%) [numbers] | |||
|---|---|---|---|---|
| Aspects of sessions | Yes | No/NR | NA | |
| Used trained faculty | 29 (40%) [19,20,23,26,28,32,33,37,38,40,41,43,44,50,51,56,58,61,63,66,67,73,75,79,85,86,88–90] | 42 (58%) [21,22,24,25,27,29–31,34,35,36,39,42,45,46,48,49,53–55,57,59,60,62,64,65,68–72,74,76,77,78,80,81,82–84,87,91] | 2 (3%) [47,52] | |
| Pre-learning materials | 21 (29%) [22,26,28,33,35,37,38,40,41,43,45,56,58,62,75–77,81,82,87,88] | 46 (63%) [19–21,23,25,27,29,30,32,34,39,42,44,46,48–51,53–55,57,59–61,63,64,66,67,68–72,73,74,78,79,80,83–86,89–91] | 6 (8%) [24,31,36,47,52,65] | |
| Didactics and Q/A | 43 (60%) [20–23,25–28,30,33–35,37,38,40,42,45,46,48,49–51,53,55,60–63,66,68,69,72,75,76–78,80,81,84,85,87–89] | 24 (33%) [19,29,32,39,41,43,44,54,56,57,58,59,64,67,70,71,73,74,79,82,83,86,90,91] | 6 (8%) [24,31,36,47,52,65] | |
| Simulation activity | 66 (90%) [19–23,25–30,32–35,37–43,45,46,48–51,53–64,66–91] | 1 (1%) [44] | 6 (8%) [24,31,36,47,52,65] | |
| Small group discussion/focused group discussions | 9 (12%) [35,45,55,60,63,76,83,84,91] | 58 (79%) [19–23,25–34,37–44,46,48–51,53,54,56–59,61,62,64,66,67–75,77–82,85,86,87–90] | 6 (8%) [24,31,36,47,52,65] | |
| Debriefing/Feedback | 21 (29%) [19,20,26,28,32,35,37,43,45,46,49,55,60,62,73,75,76,85,89–91] | 46 (63%) [21–23,25,27,29,30,33,34,38–42,44,48,50,51,53,54,56–59,61,63,64,66–72,74,77–84,86–88] | 6 (8%) [24,31,36,47,52,65] | |
| Session evaluation | ||||
| Evaluation/Assessment | 66 (90%) [19–23,25–30,32–35,37–46,48–51,53–64,66–90] | 1 (1%) [91] | 6 (8%) [24,31,36,47,52,65] | |
| Evaluation tool | In-house developed tools (42) (58%) [19,21,22,24–26,28,35,36,38,41,45,49, 51–53,57,58,60–63,65,66,68,69,71,72–81,83,84,87–89] | |||
| Standardized tools (26) (36%) | ||||
| Types of standardized tools | Simulator scoring system | 4 (5%) [34,64,70,82] | ||
| Standard guidelines/prescription | 1 (1%) [39] | |||
| Global Operative Assessment of Laparoscopic Skills (GOALS) | 3 (4%) [23,50,54] | |||
| Objective Structured Assessment of Technical Skills (OSATS) | 6 (8%) [27,29,40,82,85,86] | |||
| Direct Observation of Procedural Skills (DOPS) | 3 (4%) [37,43,50] | |||
| McGill Inanimate System for Training and Evaluation of Laparoscopic Skills (MISTELS) | 2 (3%) [56,59] | |||
| Others (reported only once) | 11 (15%) [20,31,32,33,43,44,47,55,67,82,90] | |||
| Evaluation tool reliability and validity | 38 (52%) [20,22,23,27–29,32–34,37,39,40,41,43–45,47,50–52,54–56,59,62,63,65,67,70,72,76–78,81,82,85,86,90] | 34 (47%) [19,21,24–26,30,31,35,36,38,42,46,48,49,53,57,58,60,61,64,66,68,69,71,73–75,79,80,83,84,87–89] | 1 (1%) [91] | |
Note: This table summarises the five key components of the simulation activities reported in the included studies. It also presents the evaluation or assessment tools used in the simulation sessions and the number of studies in which their reliability and validity were assessed. Several studies used multiple standardised evaluation tools. As a result, the reported numbers do not represent the total number of studies.
Each study was coded according to its central purpose, whether it introduced simulation tools, evaluated instructional effectiveness, supported faculty development, delivered teaching or explored simulation conceptually. Five themes were identified:
1.Simulation as a commodity: the first theme, simulation as a commodity, focused on reporting the effectiveness of simulation as a commodity, highlighting the development, validation or use of simulation tools, simulation techniques, simulators and simulation centres, including wet lab setups, virtual platforms and task trainers (n = 23, 31%) [19,26,39,40,42,43,46,49,51,53,56,58,66,68,70,71,73,74,77,78,80,85,91]. The individual codes included in-house task trainers [19,40,56,58,71,85], commercial simulators [26,43,68], animal cadavers [42,46,53], three-dimensional printed models [51,91], simulation space including SCIL labs [66,80], virtual simulators [70,74,77,78], simulation technique [73] and adherence to treatment guidelines in specific clinical scenarios [39].
2.Simulation as an instructional method: the second theme addressed simulation as an instructional method, focusing on evaluating it as a teaching medium for clinical skills (n = 13, 18%) [20,24,29,41,45,54,55,57,61,65,87,89,90]. The individual codes included surgical skills [24], basic clinical skills (history taking, physical examination, counselling, inter-professional communication, scrubbing, gowning, gloving and breaking bad news) [20,41,45,54,55,57,61,65,87,89,90] and non-surgical procedural skills [29,41].
3.Simulation for professional development: another group of studies focused on professional development, examining healthcare professionals’ perceptions of simulation, faculty training, postgraduate skill enhancement and clinical competence (n = 19, 26%) [21,22,27,28,32,34,35,37,38,48,50,59,60,62,72,82,83,86,88]. Individual codes included surgical skills [22,27,34,48,62,72,86], basic clinical skills (history taking, physical examination, counselling, inter-professional communication, scrubbing, gowning, gloving and breaking bad news) [21,28,32,59,60,83], non-surgical procedural skills [21,35,37,88] and resuscitation [38].
4.Simulation for teaching content to medical students: the theme of teaching content to students through simulation included simulation-based sessions aimed at perception assessment, clinical skill acquisition, procedural training and communication skill development among undergraduate medical students (n = 15, 21%) [23,25,30,33,44,52,63,64,67,69,75,76,79,81,84]. Individual codes included surgical skills [30], basic clinical skills (history taking, physical examination, counselling, inter-professional communication, scrubbing, gowning, gloving and breaking bad news) [23,25,44,52,64,67,69,75,76,79,84], non-surgical procedural skills [23,63,70,81] and resuscitation [33].
5.Simulation as a learning tool: a smaller group of studies explored simulation as a learning tool in a more conceptual sense, discussing its pedagogical value or reflecting on its integration within the curriculum (n = 3, 4%) [31,36,47]. It mainly captured perceptions, experiences and conceptual evaluations of simulation-based learning.
Across all studies, the most frequently reported outcome was Kirkpatrick Level 2 (learning/knowledge, n = 43, 58%) [19–22,25,27–30,32-35,37–40,42,45,54,55,57,58,60,62,64,67,68,70–72,75,76,80–82,84–90], followed by Level 1 (satisfaction/reaction, n = 20, 27%) [24,31,36,41,44,49,52,53,56,61,63,65,66,69,73,74,77–79,83] and less commonly Level 3 (behaviour change, n = 6, 8%) [23,26,43,50,46,59].
Tool-focused projects were mostly found in the Knowledge and Persuasion stages of adoption, while professional development and teaching content studies were more often linked to the Decision stage, where simulation use was more actively integrated. Kirkpatrick Level 3 studies tended to appear in later DOI stages (Supplementary Material Appendix D).
Overall, the findings demonstrated that intervention-based simulation projects in Pakistan are primarily situated in the early DOI stages, focusing on satisfaction, knowledge or attitude change rather than routine usage or systemic integration. Eight studies (10%) reached the Decision stage [2,5,8,25,32,33,41,73], and four (5%) showed signs of Implementation or Confirmation [28,29,30,55], indicating that only a minority of studies provided evidence of adoption decisions, sustained practice or policy-level impact. A very small cohort demonstrated what we classified as a combined Stages 4 and 5 due to a lack of clear distinction, a complex situation with fuzzy boundaries representative of real life. Examples of this process are illustrated below.
1.Knowledge: early exposure or introductory training in simulation, such as, Asif et al. [24], who introduced rectal exam training and assessed students’ learning experience (KP Level 1).
2.Persuasion: evaluation of attitudes or interest in simulation, such as, Azizi et al. [25], who conducted a POCUS workshop and assessed feedback and learning (KP Levels 1–2).
3.Decision: formal planning or piloting of simulation. For example, Bajwa et al. [26] initiated faculty development workshops (KP Levels 2–3).
4 + 5.Implementation and Confirmation: a continuum of institutional integration to sustained adoption, progressing from active integration into practice to normalised, embedded use. For example, Bajwa et al. [26] reported faculty-led simulation adaption and was therefore classified at the Implementation phase (KP Level 3). Sabzwari et al. [55] reported multi-year routine integration of moulage techniques in undergraduate assessment (KP Level 1) and demonstrated sustained practice embedded in institutional teaching. See Figure 4.
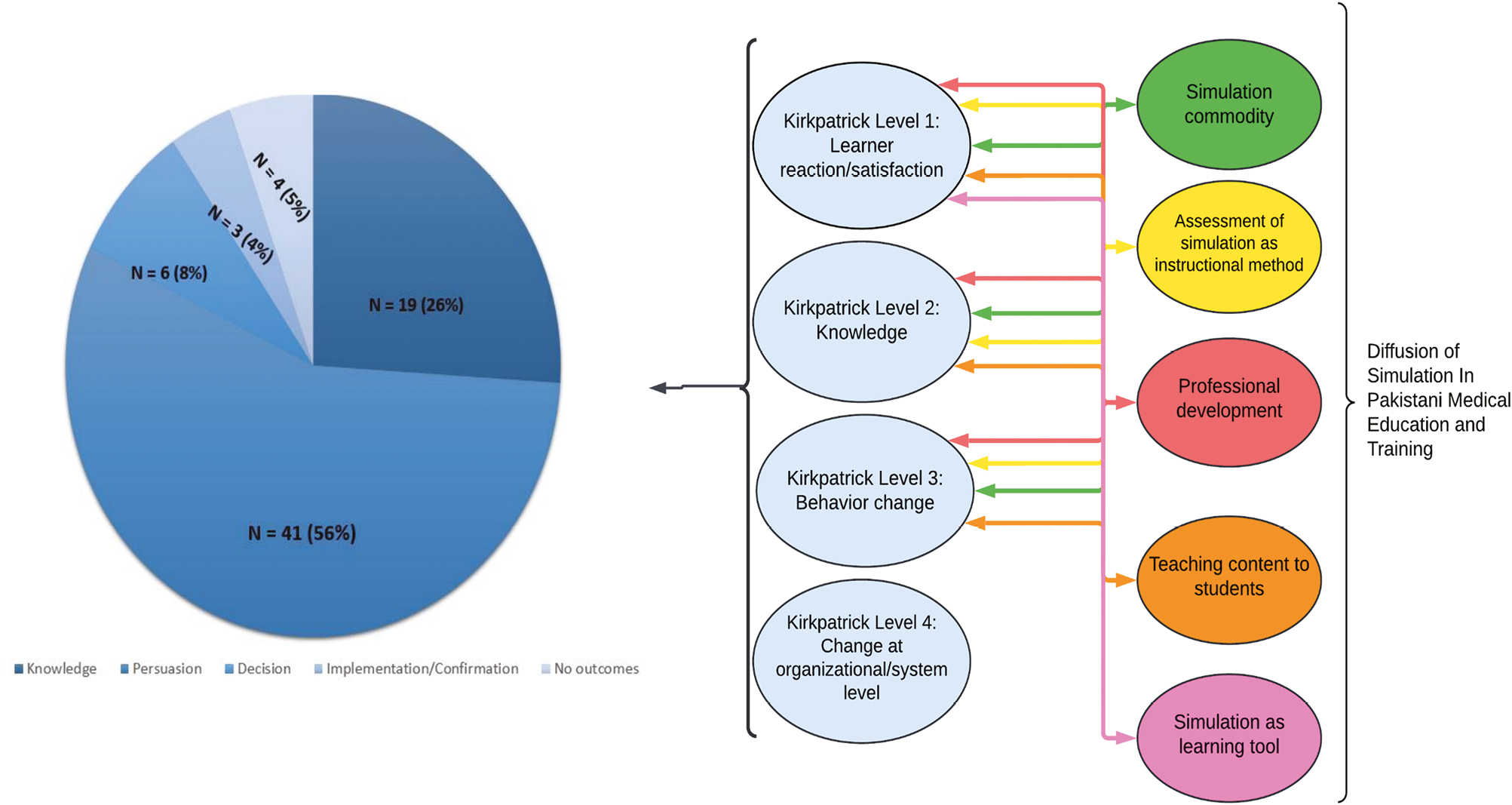
: Diffusion of simulation in medical education and training in Pakistan
A key finding was that DOI stage assignment did not always align with KP outcome measurement level. For example, Ismail et al. [25] achieved KP Level 3 (behavioural measurement) and DOI Stage 3 (Decision), indicating formal adoption planning. Conversely, Sabzwari et al. [55] reported only KP Level 1 (satisfaction) but DOI Stage 5 (Confirmation) because multi-year routine institutional use was documented. Bajwa et al. reported that their faculty development intervention achieved KP Level 3 by documenting attitude and behaviour change in participants in the follow-up survey. When participating faculty subsequently implemented simulation in their own institutional settings, that second-order adoption represented the emergence of DOI Stage 4 (Implementation).
To address the third research question, we examined the reported barriers and facilitators influencing SBE in Pakistan, focusing on how they shaped progression through the five stages of adoption: Knowledge, Persuasion, Decision, Implementation and Confirmation.
Barriers were reported in 64% of the included studies (n = 47) [19,20,22–27,30–32,35–38,40,41,44,46,47–51,55,57,60–64,66–70,72,73,75,79,81–83,85,87,88,90] and affected all DOI stages. The most cited challenges were structural: lack of funding (n = 12, 16%) [26,27,41,47,48,55,61,64,66,81,82,83] and inadequate infrastructure (n = 12, 16%) [22,24,26,40,41,46,47,55,62,79,81,83], both of which typically limited institutions to the Knowledge or Decision stages, with few advancing towards sustained implementation. In many reports, funding concerns were framed around the perceived need for high‑cost facilities and equipment, even though effective simulation can also be delivered using lower‑cost, pedagogy‑driven approaches. Human resource constraints were also noted, including limited availability of trained faculty (n = 2, 3%) [51,69] and insufficient time for simulation development (n = 4, 5%) [21,40,46,56]. These issues often disrupted progression from Persuasion to Implementation.
Technical limitations related to fidelity were another recurring theme. Anatomical inaccuracies (n = 7, 10%) [30,40,48,70,81,82,88], absence of force feedback (n = 1, 1%) [30] and inconsistent simulated patient (SP) performance (n = 2, 3%) [44,87] negatively affected learner engagement and reduced confidence in simulation as an effective educational tool. These issues commonly stalled advancement at the Implementation stage.
Barriers to Confirmation – the stage representing routine, sustained use – were less frequently reported but significant. Chief among these were limitations in outcome evaluation, including absence of long-term follow-up (n = 7, 10%) [23,25,49,60,61,72,88] and rater inconsistency (n = 7, 10%) [27,32,57,60,63,73,87], suggesting a lack of robust systems for monitoring long-term effectiveness. Notably, 34% of studies (n = 25) [21,28,29,33,34,39,42,43,45,52,53,54,56,58,59,65,71,74,76,78,80,84,86,89,91], most of which were descriptive or in early adoption stages, did not report any barriers.
Facilitators, while less frequently mentioned, were most often reported in studies situated in the Persuasion, Implementation or Confirmation stages. The most frequently reported enabler was the use of cost-effective simulation tools and techniques (n = 18, 25%) [22,26,27,29,32,40,41,42,46,48,54,56,70,72,73,77,85,88], which supported wider adoption and institutional feasibility. Experiential learning models (n = 15, 21%) [23,29,35,50,53,54,63,72,73,75,81,83,86,88,91] and access to trained facilitators (n = 6, 8%) [28,31,41,43,74,75] were also key factors, enhancing learner engagement and instructional quality – both critical for successful implementation.
Other supports included validated assessment instruments (n = 5, 7%) [20,22,40,47,54] and structured debriefing practices (n = 2, 3%) [57,75], which contributed to iterative refinement and outcome measurement, aiding progress towards Confirmation. Additional facilitators included high-fidelity simulation platforms (n = 4, 5%) [30,34,53,88], user-friendly interfaces (n = 1, 1%) [70] and portable or updatable simulators (n = 3, 4%) [48,61,88], which improved usability and scalability.
A comparative analysis revealed that studies reaching later DOI stages were more likely to report facilitators and systemic support. In contrast, those in earlier stages more often emphasised barriers or omitted contextual factors altogether. This trend suggests that the presence of enabling structures – both technical and institutional – is closely associated with successful and sustained adoption of SBE in the Pakistani healthcare context.
This PROSPERO-registered systematic review offers the first comprehensive national mapping of SBE interventions in Pakistan, guided by Rogers’ DOI framework to evaluate adoption and sustainability. Seventy-three published studies were analysed to understand the landscape, barriers, enablers and future potential for simulation in medical training, with implications for other lower-middle-income countries (LMICs) in South and Southeast Asia.
Simulation adoption in Pakistan remains fragmented, with over 80% of interventions situated in the Knowledge or Persuasion stages of the DOI framework. Most are limited to workshops, pilot sessions or partial curricular modules and report lower levels of Kirkpatrick outcomes focused on satisfaction or knowledge gains. Fewer studies in the Decision, Implementation and Confirmation stages of DOI highlight a persistent gap between innovation and institutional integration, implying that despite growing interest, simulation remains largely exploratory rather than embedded in medical education. Without strategic investment, leadership and policy support, simulation risks remaining a peripheral innovation rather than a routine educational approach.
Tools such as low-cost task trainers and in-house models were significantly more common than high-fidelity or digital modalities, which, when present, were rarely integrated into assessment frameworks or policy. Ali et al. ‘SonoGames’ [20] exemplifies purposeful adoption, showing how gamified, team-based simulation, pre-/post- evaluation and multi-institutional collaboration can enable transition into the DOI Decision and Implementation stages. These adoption bottlenecks parallel the challenges observed in other LMICs in the region, where policy ambiguity, underfunded infrastructure and fragmented leadership restrict sustainable diffusion [92]. Nagarajappa et al. report persistent infrastructure and faculty constraints in India despite national skills lab mandates [93]. Del Castillo Miranda et al. describe early-stage, low-fidelity simulation dominance in sub-Saharan Africa (Ghana, Uganda, Kenya) mirroring Pakistan’s 84% Knowledge/Persuasion distribution [94]. Southeast Asian contexts face similar policy-implementation gaps. Robinson et al.’s synthesis of 97 studies across 50 LMICs confirms Pakistan occupies a representative mid-LMIC position – excelling in low-cost innovation yet trailing high-income countries’ systemic integration [95].
Structural and human resource barriers continue to impede simulation adoption. Infrastructure and funding deficits were cited in 65% of studies; inadequate facilities, insufficient equipment and suboptimal maintenance were commonly reported. Faculty shortages and the absence of accredited, locally relevant training programmes further hinder scale-up. These systemic constraints also deepen regional disparities in access to SBE. Without targeted investment in infrastructure and faculty development, especially in underserved areas, scaling simulation nationally will remain out of reach.
Conversely, interventions supported by engaged leadership, collaborative programming and structured mentorship, such as local ‘train-the-trainer’ initiatives, were more likely to progress beyond pilot phases. Facilitators, including cost-effective simulation modalities, tailored assessment tools and local adaptation, may have contributed to wider adoption in 18 studies. The role of faculty development emerged as a specific enabler in 27% of cases. To better understand the factors influencing simulation adoption, we mapped the thematic findings onto Rogers’ five DOI attributes (Table 2). This analysis highlights that while trialability and relative advantage can support early-stage adoption, low compatibility with existing pedagogies, high perceived complexity and limited observability remain critical barriers.
| DOI attribute | Application in Pakistan’s SBE context | Impact on adoption |
|---|---|---|
| Relative advantage | Learner gains (skills, satisfaction) are reported, but system-level impact is rarely demonstrated. | Weak perceived institutional benefit limits motivation for broader adoption. |
| Compatibility | Simulation often conflicts with exam-focused, didactic teaching models. | Poor curricular fit restricts integration beyond isolated pilots. |
| Complexity | High costs, technical demands, language barriers and lack of trained faculty increase perceived difficulty. | Perceived complexity deters scale-up, especially in under-resourced settings. |
| Trialability | Pilots and workshops are common, enabling low-risk experimentation. | Encourages entry but rarely leads to sustained or formal implementation. |
| Observability | Most studies report only Levels 1–2 outcomes; few demonstrate behaviour or system-level change. | Low visibility of impact reduces leadership buy-in and policy support. |
Note: This table applies Rogers’ five DOI attributes to the context of SBE in Pakistan. The first column outlines each attribute; the second describes how it manifests within the reviewed studies; the third summarises its influence on the adoption process. The analysis is based on thematic synthesis of included studies and illustrates key factors that either enable or constrain simulation diffusion across institutional settings.
In this review, the distribution of studies across DOI stages mostly aligned with Kirkpatrick outcome levels, however, a few exceptions remained. The alignment between Kirkpatrick levels and DOI stage classification reflects the internal consistency of the mapping framework, as Kirkpatrick levels informed DOI stage assignment. However, these exceptions reveal a gap that extends beyond a measurement methodology, demonstrating that Kirkpatrick outcome levels alone are insufficient for gauging the uptake of simulation. This finding highlights SBE as a complex, real-world implementation problem requiring an implementation science framework to account for multiple contextual factors. The 84% concentration of Pakistani studies in Knowledge–Persuasion phases versus 16% in Decision–Implementation–Confirmation stages suggests structural barriers – funding, infrastructure, leadership – rather than outcome maturity alone, a phenomenon also supported by determinant theories in implementation science research on health innovation adoption in LMICs, including education contexts [96].
Late-stage progression requires organisational infrastructure and leadership alignment. Pakistan’s barriers mirror these documented systemic factors. Addressing them requires integrated implementation: simulation champions with protected time, institutional funding models and Ministry of Health guidelines embedding simulation into organisational routines. Building organisational infrastructure – the prerequisite for sustained adoption documented in implementation science – requires policy leverage. Pakistan’s regulatory structure through PMDC/HEC provides exactly this mechanism by providing the PMDC/HEC oversight on the accreditation and incentivising through regulatory requirements what otherwise relies solely on institutional initiative [5,6]. Linking SBE competencies to medical education performance expectations or accreditation criteria would distribute both mandate and resources across the medical education system – converting the competitive institutional landscape from a fragmentation risk into a coordination mechanism.
To advance SBE from early DOI stages (Knowledge/Persuasion, 84% of studies) towards sustained integration (Decision/Implementation/Confirmation, 16%), we propose consolidated, evidence-based recommendations distinguishing near-term strategies from systemic reforms. These target Pakistan’s barriers (e.g. funding and infrastructure in 65% of studies) and enablers (e.g. low-cost tools in 25%), align with DOI attributes (Table 2) and mirror challenges in other LMICs, e.g. India, Indonesia and sub-Saharan countries. National accrediting/educational bodies (e.g. PMDC/HEC in Pakistan) should lead, ensuring equitable trainee access and ultimate patient safety via Level 3+ transfer.
•Develop national accrediting bodies-recognised (e.g. PMDC/HEC) faculty training programmes (e.g. simulation educator certification pathways with CME credits and career incentives), addressing shortages and complexity for Persuasion-to-Decision shifts.
•Secure targeted hospital QA/public health funding for low-cost, scalable tools (e.g. task trainers) in rural and underserved sites (~1% training budget), tracking Level 3 Return On Investment (ROI) to enhance trialability and evidence of feasibility across South Asia.
•Standardise Kirkpatrick Level 2+ evaluations with structured simulation cases (e.g. scenario design templates, debriefing frameworks and simulation standards), improving observability where only 8% demonstrated behaviour change outcomes.
•Establish peer mentorship networks between simulation centres, leveraging the facilitators’ impactful presence documented in 25% of studies to accelerate knowledge exchange and problem-solving.
•Mandate organisational infrastructure via national accreditation standards (e.g. PMDC/HEC in Pakistan): designated simulation centres with equipment and space, trained faculty, protected coordination time and curriculum integration – ensuring infrastructure scales across institutions rather than depending on voluntary investment.
•Link SBE integration to national accreditation criteria, curriculum standards and licensing/board exam expectations (e.g. PMDC/HEC in Pakistan), embedding simulation throughout medical training and licensing pathways to create accountability for skill development from undergraduate curricula through continuing medical education for practicing physicians.
•Launch a national SBE registry tracking DOI stages, Kirkpatrick outcomes and equity metrics with benchmark capabilities, enabling donor and policy evaluation.
•Implement equity policies starting with 2–3 provincial mobile simulation units per underserved region (10–15 total initially) for targeted rural outreach, addressing geographic disparities documented across neighbouring LMICs.
•Embed SBE in national curriculum mandates with longitudinal Level 3+ research requirements, driving sustained adoption and error reduction – addressing the implementation gap documented across LMICs where most studies remain at early DOI stages.
This review has several methodological strengths. This first systematic review of Pakistan’s simulation-based medical education was registered in PROSPERO, conducted according to PRISMA guidelines and used a transparent DOI–Kirkpatrick framework to map adoption stages and educational outcomes, thereby demonstrating methodological rigour and structural coherence. The search strategy, developed with a medical librarian, encompassed multiple international and national databases with repeat search updates and no language restriction, and was paired with duplicate screening and data extraction with substantial inter‑rater agreement. Risk of bias was assessed using design‑specific JBI and NIH tools with pre-specified thresholds, critical domains and an override rule for major flaws and DOI‑stage assignments followed a transparent, step‑wise mapping procedure combining thematic analysis and Kirkpatrick‑level coding, supporting reproducibility despite heterogeneity in primary study designs and outcomes.
This review is limited by its reliance on indexed literature, which may overlook local, unpublished initiatives. DOI- and Kirkpatrick-level assessments depend on available outcomes, potentially introducing publication or reporting bias. The review did not include grey literature due to resource and time constraints of the volunteer research team, which may have led to the omission of non-indexed or institutionally archived studies, although comprehensive multi-database searching and manual reference screening helped mitigate this risk. In addition, DOI-stage and risk of bias assignments involved interpretive judgement, despite the use of pre-specified decision rules and should be viewed as structured approximations rather than definitive categorisations. Furthermore, because DOI-stage classification incorporated Kirkpatrick outcome levels as a criterion, the observed alignment between stages and outcomes reflects methodological consistency rather than an independent empirical relationship, limiting causal inference about diffusion progression.
SBE in Pakistan and its regional LMIC peers is at an inflection point. Transitioning from scattered innovation to routine practice will require robust national policy, strategic investment, empowered faculty and standardised, outcome-driven evaluation. By centring equity, scalability and measurable results, SBE can become a vital component of health workforce development and medical educational reform throughout South and Southeast Asia.
We acknowledge Dr Fouzia Sadiq, Dr Haneen Alnazawwi, Miss Jessica Bell, Dr Mustafa Naqvi and Mrs Ayesha Ayub for their support and contributions to data extraction for this project. We cordially thank Dr Suzan Kardong-Edgren for reviewing this article and providing valuable insights that improved this article immensely.
MB conceived and designed the study; led protocol development; conducted and supervised screening, data extraction, DOI–Kirkpatrick mapping and risk-of-bias assessment; synthesised findings; and drafted and revised the manuscript. FN refined the design and protocol; assisted with search strategy, screening, data collection and interpretation; and contributed to drafting and critical review. NF conducted data extraction, contributed to descriptive analysis and supported drafting, editing and critical review.
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
All data relevant to the study are included in the article or uploaded as supplementary information.
Patients or the public were not involved in the design, or conduct, or reporting or dissemination plans of our research hence no ethical approval or consent was required.
All authors have completed the ICMJE uniform disclosure form and declare no competing interests.
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
36.
37.
38.
39.
40.
41.
42.
43.
44.
45.
46.
47.
48.
49.
50.
51.
52.
53.
54.
55.
56.
57.
58.
59.
60.
61.
62.
63.
64.
65.
66.
67.
68.
69.
70.
71.
72.
73.
74.
75.
76.
77.
78.
79.
80.
81.
82.
83.
84.
85.
86.
87.
88.
89.
90.
91.
92.
93.
94.
95.
96.
 Mapping the diffusion of innovation in medical simulation in Pakistan: a systematic review
Mapping the diffusion of innovation in medical simulation in Pakistan: a systematic review
 Facebook
Facebook
 Twitter
Twitter
 Linkedin
Linkedin
 Whatsapp
Whatsapp
