
Danielle Gardner 1
ORCID:https://orcid.org/0009-0006-4901-8684
, Elizabeth Brogan 1ORCID:https://orcid.org/0000-0001-7790-6343
, Tracy Levett-Jones 1ORCID:https://orcid.org/0000-0003-4279-8957
[1]
AI chatbot,communication skills,conversation agents,manikins/mannequins,nursing education,and simulation
Article Type: brief-report
It is known that with manikin-based simulation there is often limited authentic feedback granted in response to learners’ actions. This can reduce students’ opportunities to learn from any immediate patient reactions, and lessen flexibility in their decision-making [1].
Conversational agents (CAs) colloquially known as ‘chatbots’, are AI-driven units designed to engage in human-like conversations. When used in an educational setting, these chatbots can provide learners with interactive support by delivering natural responses and provide more authentic conversational experiences [2].
Traditional simulation-based learning (SBL) often lacks genuine real-time responsiveness, which may limit the experience, reducing student engagement and motivation [3]. SBL offers students opportunities to develop their technical skills in simulated settings; however, teaching non-technical skills such as empathy, critical thinking, clinical reasoning and time management can be challenging. Alternatively, AI chatbots can provide a realistic ‘patient’ voice for manikins, which has the potential to overcome several of these concerns and may result in a more engaging and authentic learning experience.
As part of a Teaching and Learning project, a cross-disciplinary team from the faculties of Health and Engineering at the University of Technology Sydney collaborated on a pilot study to determine the feasibility of a scalable communication skills training platform called SimConverse. This AI-generated chatbot allows learners to participate in therapeutic conversations with a simulated patient. The platform allows for scaffolded learning that supports communication and clinical reasoning, so that healthcare students can practise and refine their ‘non-technical’ skills in a safe, secure environment.
When used at the bedside in the simulation setting, this AI-generated conversation agent serves as the voice of a manikin-based ‘patient’, enabling students to engage in meaningful, authentic and therapeutic conversations whilst providing clinical care.
The innovation was implemented with groups of first-year Bachelor of Nursing (BN) students who were required to engage with simulated patients over a 4-week period. Students were required to learn, practise and perform a series of nursing skills on the manikin-based patients each week.
When interacting with the manikin patients, the main ‘non-technical’ criteria for students to address involved gaining consent and providing explanation and reassurance whilst attending to the prescribed assessments and procedures.
At the end of the teaching period, we surveyed student satisfaction with the use of conversation agent technology using the Simulation Satisfaction Experience Scale (SSES). Figure 1 represents levels of students satisfaction measured via a 9-item instrument using a Likert scale of strongly agree to strongly disagree [4]. The final item included a series of open-ended questions that asked students to provide further feedback on their experience. Additional data sought from interactions between the students and the AI manikin was collected using direct observation via audio-visual footage captured by Learning Space technology, and voice transcripts generated from the SimConverse Platform itself. Evaluation of this data allowed us to make improvements to the system, allowing for a smoother and more authentic experience when interacting with the AI-generated manikin patient.

![Graph of overall positive responses to students’ perceptions of their clinical reasoning and clinical learning post-intervention with AI conversation agent (SSES) [4]](/dataresources/articles/content-1780059613150-ece3c05b-e54a-4f41-8b14-02714a25452a/assets/xeyw9498_f0001.jpg)
Graph of overall positive responses to students’ perceptions of their clinical reasoning and clinical learning post-intervention with AI conversation agent (SSES) [4]
Data from the SSES [4] indicates that students saw the intervention as a positive learning experience overall, with more than 70% of the positively worded statements answered as either agree or strongly agree.
Feedback from the open-ended questions identified that the students found the experience to be immersive and realistic. Many students commented that they felt the experience enhanced their confidence with patient communication, that they felt less awkward speaking to CA manikins, and that this improved their responses to the patient.
Negative feedback mostly related to misunderstandings from the CA if it did not understand what the student was saying. During one encounter the chatbot appeared to get ‘annoyed’ by a student when it did not understand; however, staff transformed this into a learning opportunity during the debrief session when discussing communication barriers. We also learned to appreciate that it is not necessary to control every word from the chatbot, as conceptual standardization gave varied responses each time, demonstrating its linguistic flexibility.
Potential infection control issues were identified with the initial set-up, as the PC is controlled by pressing the spacebar to activate the voice recognition technology, and students were touching the PC whilst performing their skills.Engineering adaptations included installing foot pedals around the bedspace thatallow students to activate the chatbot hands-free, eliminating the need to touch the PC with gloved hands (Figure 2).
The microphone system was upgraded with two transmitters at either end of the bed and one receiver by the PC. This addressed difficulties in picking up student speech, especially in a noisy environment (Figure 2).
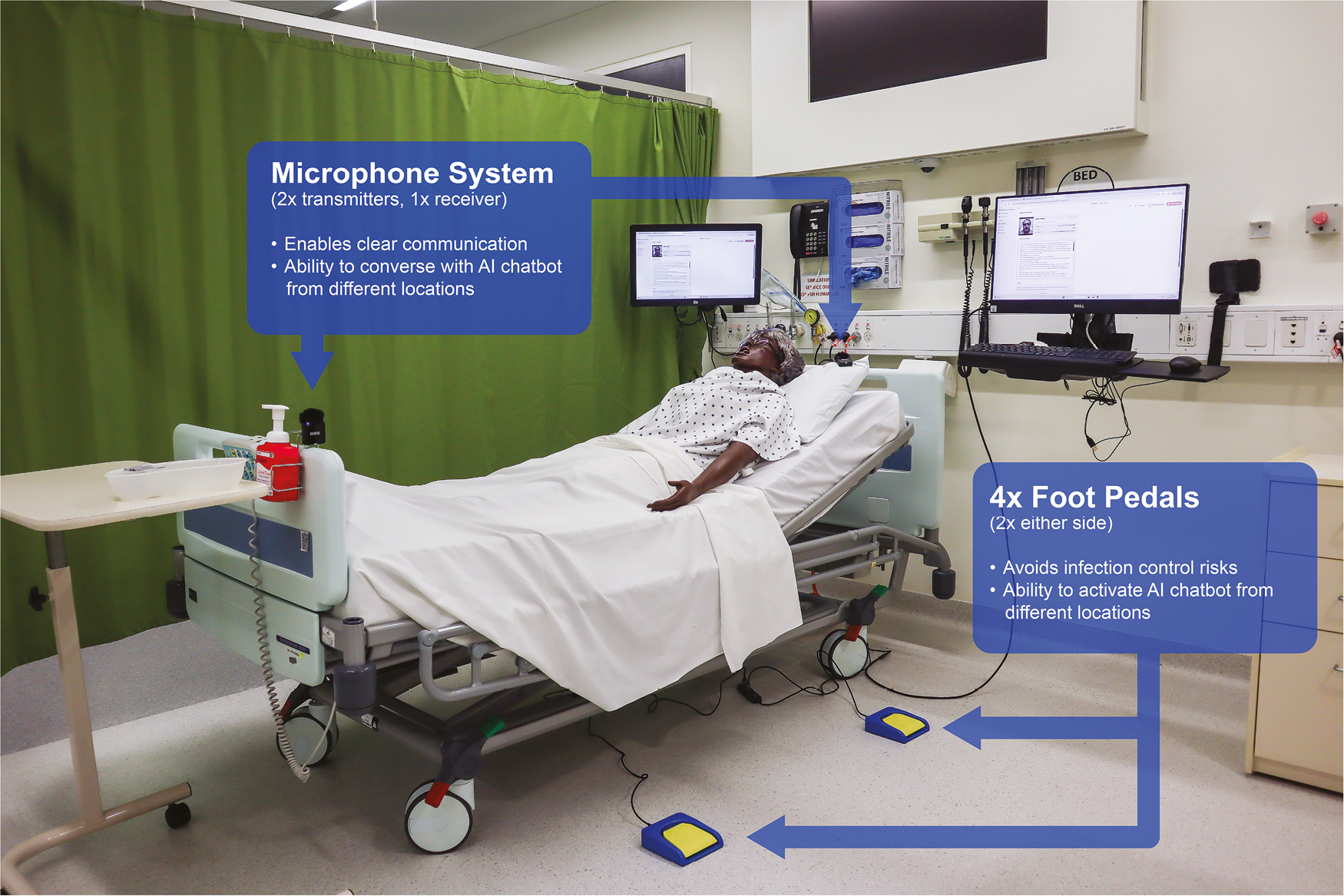
Conversational agent bedspace set-up in the Clinical Simulation Laboratories – University of Technology Sydney
The innovation will be implemented into the UTS BN curriculum in upcoming semesters and the authors plan to study the effect this innovation has on the communication confidence of first-year students prior to their first clinical placement. Further research involves a mixed-methods study using the intervention in an objective structured clinical examination scenario to compare the use of conversational agents between groups.
The authors would like to acknowledge Professor Stuart Perry and Marie Aguinaldo from the UTS Faculty of Engineering and IT; Thomas Lo, Shannon McFarlane, Erica Calderone and the UTS Faculty of Health Simulation Laboratory team; and Patrick Abela from the UTS Faculty of Health Teaching and Learning Department for their contributions to this project.
None declared.
None declared.
None declared.
None declared.
The authors have no conflicts of interest relevant to this article to disclose.
1.
2.
3.
4.
John T. Paige 1
ORCID:https://orcid.org/0000-0002-7309-6520
, Kathryn Kerdolff 1ORCID:https://orcid.org/0000-0001-8392-1830
, Deborah Garbee 2ORCID:https://orcid.org/0000-0002-3428-5337
, Qingzhao Yu 3ORCID:https://orcid.org/0000-0001-8194-0798
, Laura Bonanno 2ORCID:https://orcid.org/0000-0002-2586-1195
[1]
[2]
[3]
assessment,innovation,interprofessional education,simulation,and teamwork
Interprofessional education (IPE) high-fidelity simulation (HFS) training is an effective means of developing teams for today’s demanding healthcare environment. Its success depends on the reliable, effective and efficient measurement of teamwork for accurate assessment of gaps in performance. Although survey- and observer-based teamwork instruments exist with evidence of validity for a wide variety of targeted populations [1,2], their inaccuracy in assessing teamwork continues to pose a problem due to observer biases and subjectivity. To date, quantitative measures of teamwork skills in healthcare are still lacking. To address this issue, the authors have worked on conceptualizing how to incorporate quantitative measurements into IPE HFS [3]. This report focuses on the pilot implementation of volume measurement using dosimeters as a potential component for the quantitative measurement of teamwork.
For conceptualization of a quantitative measurement suite of team performance, the authors [3] used Luciano et al.’s [4] framework, incorporating construct, measurement and context components. The TeamSTEPPS™ dimensions of leadership, communication, situation monitoring and mutual support served as the teamwork construct [5]. For the communication dimension, voice quality reflected through voice volume served as one measurement using a dosimeter as the means for its assessment. Contextually, the dosimeter provided a means of evaluation in multiple environments (i.e. clinical, HFS, experimental) due to its portable nature and ease of data collection.
Pilot implementation of the dosimeter occurred as part of student operating room team training (SORTT) sessions, a programme involving HFS IPE of senior undergraduate nursing students, senior medical students and nurse anaesthesia students. These sessions involved a dual scenario, intraoperative crisis-based format with immediate after-action debriefing on team-based competencies. Two separate dosimeters measured OR volume, one placed near the head and foot of the ‘patient’s’ bed, respectively, as illustrated in Figure 1.

Positioning of dosimeters near the head and foot of the OR table during SORTT to measure voice volume. Dosimeters are circled in the figure
Evaluation involved a quasi-experimental, pre-/post-intervention design comparing the mean dosimeter results from the head of the bed, from the foot of the bed and combined for each scenario. In addition, observer-based teamwork assessments for each scenario involved the use of the Quick Teamwork Assessment Scales (Q-TAS), a 5-item instrument using a 6-point Likert-type scale (1 = definitely no to 6 = definitely yes) and having three subscales (team-based behaviours [TBB, two items], shared mental model [SMM, one item] and adaptive communication and response [ACR, two items]). Paired t-test scores compared mean scores for the dosimeter values and Q-TAS scores, with a threshold of p < 0.05 for significance.
Available data from 2020 SORTT sessions involved eight teams for dosimeter measurements and seven teams for Q-TAS assessments. Table 1 lists dosimeter scores for the head of the OR table, foot of the OR table and combined. Although not significant, all dosimeter values increased from scenario one to scenario two. All Q-TAS subscale scores from scenario one to scenario two had statistically significant increases, indicating an improvement in team function.

The lack of significance for the dosimeter scores could be related to the nature of how volume measurements were made during the SORTT sessions. The dosimeter collected measurements at set time intervals throughout each scenario, and these intervals did not necessarily correspond with start and stop times for a scenario. Thus, alignment of dosimeter values with the exact timing of each scenario did not occur, necessitating estimation of starting and stopping volume measurements in cases of overlap between dosimeter measurement intervals and the beginning and ending of a scenario.
The data demonstrate that the use of dosimeters during IPE HFS is feasible from a technical standpoint. Challenges include aligning interval decibel measurements with scenario chronology to gain accurate, reliable timing of volume fluctuations during training. Seamless synchronization of the start and stop of dosimeter measurement with the onset and conclusion of each scenario requires further development.
Additional next steps include merging dosimeter values with other measurements such as team member movement, face-to-face time and speech utterances to construct a comprehensive evaluation of teamwork. Finally, aligning quantitative assessments with specific teamwork dimensions is necessary for a granular evaluative mechanism that individualizes gaps in team performance to tailor a team member’s training.
The authors would like to acknowledge the senior undergraduate nursing, senior medical and nurse anaesthesia students whose participation in and learning from the SORTT sessions provide the inspiration and motivation for our work.
All authors contributed to the conceptualization, implementation, analysis and reporting of this work.
Support for this work was through a 2019–2021 International Association of Medical Science Educators (IAMSE) Educational Scholarship Grant. Support for Q-TAS development was through a 2016–2018 Southern Group for Educational Affairs (SGEA) Medical Education Scholarship, Research and Evaluation (MESRE) Grant.
None declared.
This work was part of a larger IRB-approved exempt project looking at IPE HFS in healthcare.
Drs Paige, Garbee and Bonanno are co-editors of a book on interprofessional simulation-based training. Dr Paige is also a co-editor on additional books on simulation in radiology and surgical education. He is a senior editor for the Journal for Simulation in Healthcare.
1.
2.
3.
4.
5.
Simon Modra 1
ORCID:https://orcid.org/0000-0003-1980-2364
, Mark Billinghurst 1ORCID:https://orcid.org/0000-0003-4172-6759
, Peter Schumacher 1ORCID:https://orcid.org/0000-0001-7598-5930
[1]
anthropometry,human-centred design,simulation tools,usability,and virtual reality
Designing human spaces in high-stakes environments – such as submarines, hospitals and disaster response units – presents unique challenges due to isolation, confinement and operational pressures. These settings require environments that support complex workflows, accommodate critical equipment and ensure safety and comfort under demanding conditions. Traditional design methods, relying on sketches or static renderings, often fail to capture the lived experience of users or the operational realities of these spaces [1]. There is a clear need for innovation in design processes that prioritize human factors, usability and iterative user engagement.
High-stakes environments are defined by their extreme constraints: limited space, high operational demands and the need for continuous human performance under pressure. The consequences of design failure in these contexts can be severe, impacting safety, efficiency and wellbeing. Therefore, a robust, user-centred approach is essential to ensure that spaces are not only technically sound but also genuinely fit for purpose.
We developed and implemented a simulation-integrated human-centred design (HCD) methodology tailored for high-stakes environments. Our approach embeds virtual reality (VR), augmented reality (AR), mixed reality (MR) and physical prototyping into each phase of the design process. This layered use of simulation tools enables immersive user engagement, rapid prototyping and iterative feedback, ensuring that design solutions are grounded in real-world needs.
The process begins with broad contextual research and low-fidelity prototypes – such as VR walkthroughs and physical maquettes – to explore spatial relationships and user behaviours. Insights are synthesized into design criteria using Digital Human Mannequins (DHMs) and scenario mapping. Multiple design proposals are then developed and tested with end users using a combination of VR simulations, physical mock-ups and CAD analysis [2]. The final phase delivers high-fidelity outputs, including refined CAD models, immersive VR environments and full-scale prototypes for stakeholder validation [3].
A key innovation is the use of ‘negotiotypes’ – deliberately unresolved models, both physical and digital, designed to provoke structured user feedback and encourage co-creation. By embracing imperfection, these models foster deeper engagement and help surface latent needs and preferences that might otherwise remain hidden.
Impact was measured through structured evaluation sessions with end users, including military medics, hospital staff and operational planners. Methods included ethnographic observation, user interviews, focus groups and usability testing [4]. Each simulation modality – VR, physical mock-up, CAD – provided unique insights, and feedback was mapped against design criteria to ensure traceability and alignment with operational requirements.
Quantitative data were collected through task performance metrics, spatial analysis and ergonomic assessments using DHMs. Qualitative data were gathered from user feedback during immersive workshops and participatory design sessions. This mixed-methods approach allowed for a comprehensive evaluation of both functional and experiential aspects of the designs.
Two case studies illustrate the effectiveness of our approach:
1.Deployable Medical Life Pod:
A multi-modal simulation strategy was used to design and validate a compact medical capsule for field deployment. Full-scale physical mock-ups, VR simulations and scale models (Figure 1) enabled stakeholders to interact with the design, identify spatial constraints and refine workflows. Feedback from end users led to iterative improvements, ensuring the pod’s suitability for rapid deployment and medical intervention.
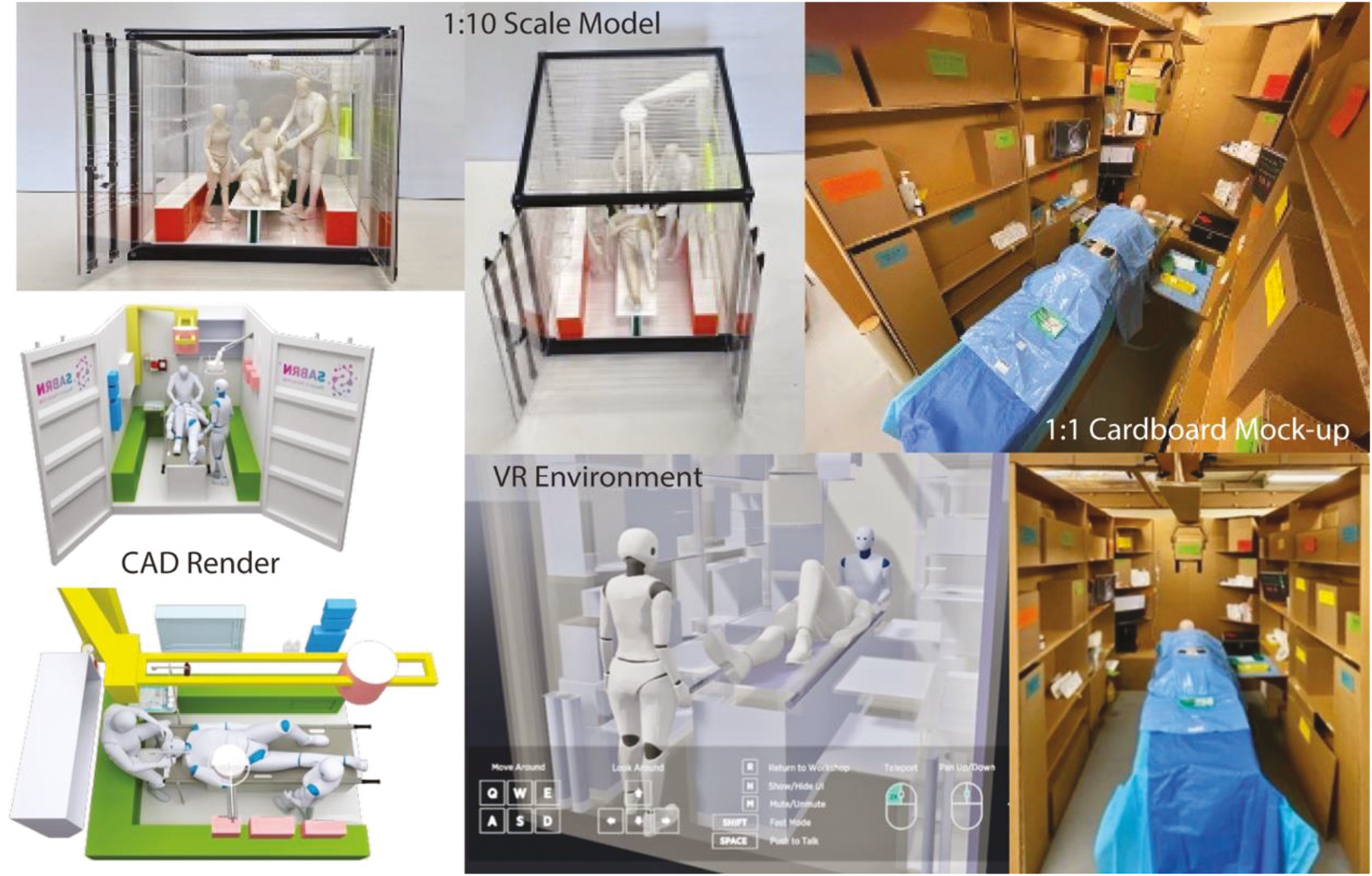
Four different modelling techniques used for SABRN
The use of layered simulation tools allowed for early identification of ergonomic issues, improved equipment layout and optimized patient care pathways. The final design was validated through immersive VR scenarios and hands-on evaluation with medical personnel, resulting in a solution that balanced technical requirements with human factors.
2.Hospital Room Sizing Validation:
For the New Women’s and Children’s Hospital, full-scale cardboard mock-ups of key clinical spaces were constructed (Figure 2). Immersive workshops with hospital staff revealed critical shortcomings in proposed room sizes and configurations, leading to a redesign of the facility before construction. This participatory approach prevented costly downstream revisions and ensured the new hospital would meet operational needs.
The process highlighted the value of engaging end users early and often, using tangible prototypes to surface latent design issues and facilitate collaborative problem-solving.
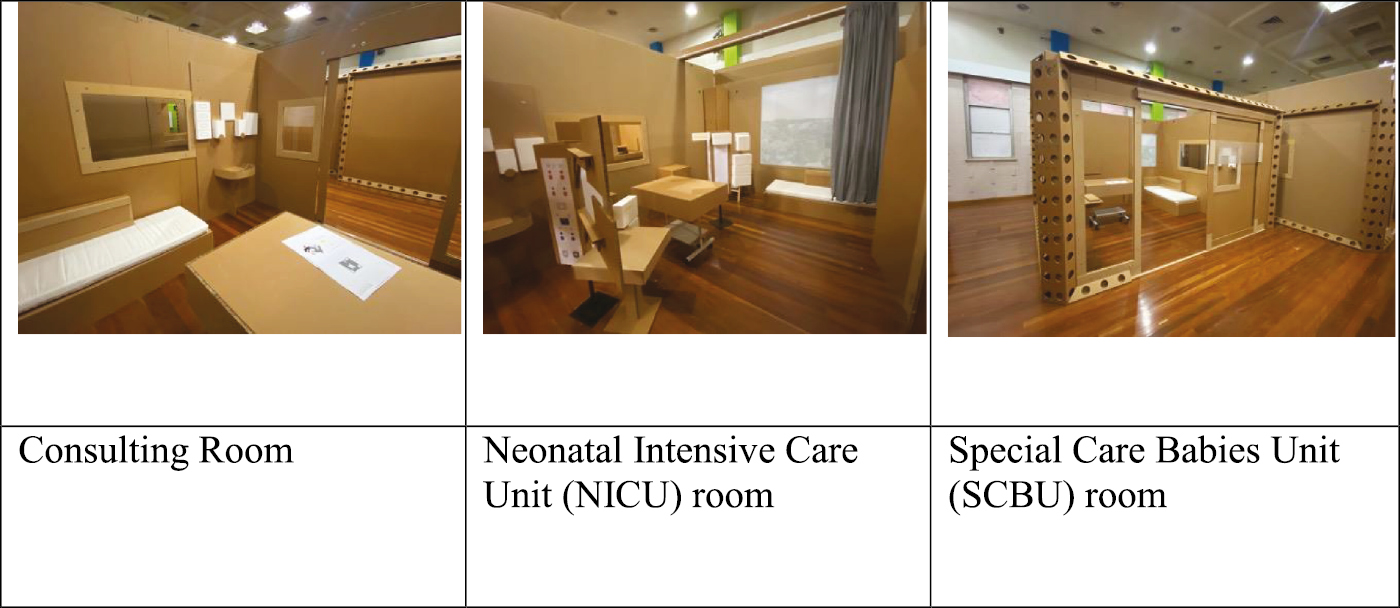
1:1 Mock-ups of different room designs for the Adelaide New Women’s and Children’s Hospital
•Layered simulation is essential for holistic understanding.
•Early prototyping reduces downstream risk.
•Stakeholder engagement drives relevance and usability.
•Tool fluency enhances adaptability.
•Simulation fidelity should match the design phase.
Future research should focus on integrating AI-assisted design tools for automated simulation setup and analysis, real-time data integration for adaptive environments and digital twin frameworks for continuous validation. Developing scalable evaluation methods will further enhance the impact of simulation tools across diverse domains. As simulation technologies evolve, their integration into HCD processes will be critical for designing environments that are both technically robust and deeply aligned with human needs.
There is also a need to address current limitations, such as the resource intensity of high-fidelity physical mock-ups and the interoperability challenges between VR and CAD platforms. Exploring new methods for real-time model manipulation within immersive environments and expanding the use of digital twins for ongoing validation, will be important areas for future investigation.
None declared.
None declared.
None declared.
None declared.
None declared.
1.
2.
3.
4.
Belinda Judd 1
ORCID:https://orcid.org/0000-0002-6640-269X
, Kelly Squires 2ORCID:https://orcid.org/0000-0003-2080-3102
, Tayne Ryall 3ORCID:https://orcid.org/0009-0004-6246-5812
, Christie Van Diggele 1ORCID:https://orcid.org/0009-0005-9437-5800
, Kellie Britt 4ORCID:https://orcid.org/0000-0003-2735-9446
, Pauletta Irwin 5ORCID:https://orcid.org/0000-0003-3242-4273
[1]
[2]
[3]
[4]
[5]
education,health professions education,interprofessional education,realism,fidelity,authenticity,and simulation
Interprofessional education (IPE) is increasingly recognized as essential for preparing collaborative health professionals capable of delivering safe, quality, team-based care. IPE describes students or professionals from two or more disciplines learning with, from and about each other to improve collaboration and quality of care. Shared learning proposes to facilitate inclusive and collaborative practices, a greater understanding of one’s own professional identity and the role of self and others within the healthcare team. Simulation-based approaches are recommended by bodies such as the World Health Organization (WHO), publishing global guidelines advocating for embedding IPE experiences within health curricula to enhance workforce readiness [1]. However, tertiary institutions often cite faculty training gaps, logistical complexities and constrained resources as barriers to authentic, scalable IPE implementation [2].
In response, a national team from the Australian Society for Simulation in Healthcare (ASSH) developed an online, cross-institutional simulation programme to pilot a scalable IPE model. Our aim was to evaluate its feasibility and potential to foster student professional identity and teamwork skills ahead of broader deployment.
We conducted two consecutive pilot iterations involving pre-registration students from nursing, pharmacy, physiotherapy, dietetics, social work and medicine across multiple Australian universities. The programme design was adapted from a single-institution initiative [3]. Voluntary student recruitment was enabled through institutional communications. Simulated patients were employed to portray the patient cases through recorded vignettes.
Case development involved a reference group of 11 expert clinicians (covering seven professions – Table 1), who reviewed draft cases for realism, complexity and relevance. Final cases featured both a simulated patient vignette and a written case history. All materials, including cases, objectives, rubrics and simulated patient vignettes were available to students on an online structured Microsoft Teams™ site. Students worked in small interprofessional groups to develop and present interdisciplinary management plans via video or written submissions. Following the activity, educators provided structured, purposeful feedback on each team’s submission to enhance learning and reflection.
| Development phase | Pilot 1 | Pilot 2 | Total (n =) | |
|---|---|---|---|---|
| Reference group - expert clinicians | Occupational therapy – 1 Physiotherapy – 3 Dietetics – 1 Social work – 2 Nursing – 2 Medicine – 1 Speech pathology – 1 |
11 | ||
| Student participants | Nursing – 3 Pharmacy – 2 Physiotherapy – 3 |
Physiotherapy – 7 Dietetics – 6 Social work – 6 Medicine – 1 |
28 |
In a mixed-methods approach, students completed pre- and post-questionnaires including the Professional Identity Scale, the Team Scale and the Cognitive Flexibility Scale [4]. Students also participated in post-programme online focus groups to explore their experiences qualitatively. The results informed feasibility, acceptability and the programme’s preliminary impact on professional identity and collaboration skills.
The pilot cycles engaged 28 students across six disciplines (Table 1).
Students valued the experience.
It would be great to have this interprofessional team building as a compulsory course prior to placement (P1SW2)
This exercise really reinforces my understanding and the belief that the care program is really an integrated and comprehensive activity (P2NU1)
Students were engaged.
I felt part of the team and the decision making (P2DI2)
I thought the video was very immersive in the sense that it felt very real (P1NU2)
Students saw it as an opportunity to learn about professions that they knew very little about.
… but physiotherapy, I don’t have any knowledge about what they do or what they can do (P1PH1)
Despite small numbers, early findings from the pre- and post-questionnaires suggest this programme enhanced enjoyment of working in a team environment, further developed teamwork skills, improved participants’ ability to communicate their ideas in peer collaboration and strengthened participants’ connection with their profession.
IPE was highly valued by all involved and recommended to be integrated into all pre- and post-health professional curricula. The cross-institutional nature of the programme improved accessibility to IPE for learners across metropolitan, regional and rural areas, and added additional benefits to learning and engagement. This small, low-resource programme has the potential to broaden to a large-scale and may be suitable for developing professional identity and multidisciplinary teamwork skills. The model proved low-cost, requiring no physical lab space and minimal faculty time, primarily focusing on case development and feedback delivery. A larger effectiveness trial is needed to measure professional identity, interprofessional attitudes and cognitive flexibility. Future iterations may also consider further augmented reality or live virtual simulation to enhance learning outcomes.
All authors contributed to conceptualization, data collection, analysis and writing of the study.
This work was supported by funding from Simulation Australasia, the Britt Family Trust and a Teaching Innovation Generating Education Research (TIGER) grant from the University of Canberra.
None declared.
Ethics approval was granted by the Human Ethics Committee of the University of Canberra (Project 11827). Voluntary, informed written consent was granted by all participants prior to inclusion in the study.
None declared.
1.
2.
3.
4.
Elise Sutton 1
ORCID:https://orcid.org/0009-0003-8910-0445
, Kirin Channa 1, 2ORCID:https://orcid.org/0009-0008-5800-5812
[1]
[2]
Emergency Department,healthcare systems,human factors/ergonomics,in situ simulations,occupational violence and aggression,OVA),Quality and Safety,quality improvement,Safety-II,and translational simulation
Healthcare is a complex system requiring resilience, adaptability and variation [1]. However, safety improvement work in healthcare traditionally relies on a top-down approach focusing on work-as-imagined/prescribed rather than the practicality of work-as-done [1,2]. This disconnect results in variation as healthcare workers adapt to complete a necessary task [1,2,4].
Translational simulation (TS) is a tool utilized in healthcare to directly improve patient care and healthcare systems, whilst delivering simulation-based interventions [3]. TS supports systems testing and embeds good practice to build organizational resilience, aligning with Safety-II principles – learning from normal work and guided adaptability [2]. Acting as a proxy for work-as-done, TS enables staff to diagnose latent system threats, improve teamwork and identify problems and solutions not apparent through traditional approaches [4].
Occupational violence and aggression (OVA) is a growing global health issue, negatively impacting well-being of healthcare workers and contributing to poor quality patient outcomes and increased system costs [5].
Following an increase in OVA events at a busy Emergency Department (ED) in Melbourne’s North, the Executive team engaged the local Simulation and Safety team (SAS) who specialize in TS, to further investigate and diagnose system-level issues. SAS predominantly conduct in situ simulations in the clinical environment to maximize testing of the systems, equipment and inclusion of end-users who do the actual work.
Unlike prior serious OVA simulations with offenders wielding a weapon which were conducted in unoccupied clinical spaces, the TS activity described in this paper was specifically designed to be conducted in a live patient environment requiring extensive planning and communication. Pre-briefing involved staff meetings and e-mail promotion, plus multilingual brochures, signage and overhead announcements for Consumers. Given the exceptionally dynamic and unpredictable setting of ED, additional safety measures were implemented including observers assigned for the simulated patient (SP), monitoring for real OVA events, local communication, crowd control, patient experience and oversight of staff well-being by a Psychologist.
The simulation commenced inside the ED with the SP becoming aggressive whilst wielding a pole before progressing to the Ambulance Bay and further threatening staff and damaging property. The SP wore a clearly marked ‘ACTOR’ T-shirt to differentiate them from a real aggressor. The ED and Security teams retreated inside and awaited the simulated arrival of Victoria Police, where the scenario concluded with the simulated use of capsicum spray.
A 90-minute debrief followed, attended by 32 participants including representation from ED, Occupational Health and Safety, Emergency Management, Mental Health, Security, Ambulance Victoria and Victoria Police. The debrief allowed extensive discussion of the scenario, reflection of recent events and identification of systems vulnerabilities. Fifteen recommendations were developed to mitigate threats and enhance systems and team resilience (see Table 1). Recommendations included two space-related recommendations, one staff-related recommendation related to acknowledging the fight/flight/freeze response, three relating to equipment and nine systems focused recommendations. Recommendations were presented at the Quality and Safety Committees to ensure organizational oversight and follow-up.
| Recommendation | Focus type | Strength of recommendation | Impact |
|---|---|---|---|
| Capital team to consider need for higher desks within the ED. | Space | Strong | Divisional |
| ED Leadership team to review which group would be best placed to conduct safety walkarounds and embed this into regular duties. | Space | Weak | Local |
| OVA training to include acknowledgement of fight/flight/freeze response. | Staff | Weak | Organizational |
| Engineering to review external Ambulance Bay doors to determine if there is a fault with the bottom part of the door. | Stuff | Strong | Divisional |
| Emergency Services Leadership to review replacing Ambulance bay doors with higher grade glass. | Stuff | Strong | Divisional |
| Ambulance Victoria (AV) to provide additional training regarding the use of duress for OVA incidents within hospital settings and encourage use. | Stuff | Weak | External |
| Implementation of overhead hospital-wide chimes announcement of all OVA events involving a weapon. | Systems | Strong | Organizational |
| OVA trainers and ED Leadership to: a) Benchmark with external Emergency Services regarding role allocation during OVA situations. b) Review and update training and procedures to reflect team approach. c) Pre-allocate roles at beginning of shift. |
Systems | Moderate | Organizational |
| Script for Emergency Services for OVA event with weapon involvement. a) Victoria Police (VicPol) to share Emergency Services Telecommunications Authority (ESTA) script for violence and aggression with the healthcare organization. b) Script to be incorporated into the local healthcare organizations procedure and training. c) ED Leadership to ensure script is readily available to staff escalating OVA with weapon event. |
Systems | Moderate | Organizational |
| Review script for communication staff to ensure caller activating OVA event with weapon is asked if it is safe for them to remain on the line to talk to ESTA. | Systems | Moderate | Organizational |
| Consider options of notifying AV staff within the Ambulance Bay of safety incident: a) Installation of speaker within Ambulance Bay. b) Installation of light/beacon. |
Systems | Strong | Divisional |
| VicPol to explore notification of OVA with weapon event to AV crews in the area through ESTA. | Systems | Moderate | External |
| Executive and Legal teams to raise the discussion of Protective Services Officers (PSO) in hospitals at government level. | Systems | Moderate | External |
| ED Leadership to provide additional training to staff regarding the process of lockdown and evacuation. | Systems | Weak | Local |
| Increased Security monitoring of the Ambulance bay in the subsequent hour(s) post planned eviction. | Systems | Moderate | Divisional |
SAS collated a comprehensive simulation report detailing the simulation, timeline, key discussion points and recommendations. Recommendations are allocated a focus type – space, staff, stuff, systems or other; recommendation strength – weak, moderate or strong; and impact – local, divisional, organizational or external (see Table 1 for list of recommendations). The debrief and feedback highlighted the persistent gap between work-as-imagined and work-as-done, reinforcing the value of TS in identifying and addressing this gap.
Utilizing TS to act as a proxy for work-as-done in an OVA event allowed for identification of areas of inevitable variation from work-as-prescribed/imagined. The team was able to facilitate and encourage learning from this variation and develop recommendations derived from actions staff members naturally took to bridge the gap between work-as-imagined or prescribed and what was practical in the situation. There was collaboration between managers and frontline workers to diagnose latent threats and to establish possible mitigation strategies. The simulation demonstrated the different fight, flight or freeze responses staff face in the face of fear. The debrief displayed an enhanced understanding by leadership and non-clinical staff of the challenges end-users often face and an increased appreciation of the cognitive and emotional responses staff manage during violent events.
Recommendations did not focus on individual performance, rather they focused on human factors and the engineering of systems and design. Conducting the OVA simulation really highlighted the issue but also emphasized the commitment the organization has to work collaboratively with the end-users. This work demonstrates the value of TS for system improvements around OVA, and how to achieve in situ simulation using simulated patients in a live clinical environment. SAS will utilize learnings from this TS to inform future OVA TS in different environments including Mental Health and General Acute Adult wards.
None declared.
None declared.
None declared.
Quality Assurance was obtained at Northern Health in accordance with the National Statement on Ethical Conduct in Human Research (2023), NHMRC Ethical Considerations in Quality Assurance and Evaluation Activities, and institutional guidelines. Reference number QA 10.2025.
None declared.
1.
2.
3.
4.
5.
Pauletta Irwin 1
ORCID:https://orcid.org/0000-0003-3242-4273
, Amy Barnett 1ORCID:https://orcid.org/0009-0009-0429-9584
[1]
educational design,innovation,nursing education,simulation,technology,and translational simulation
Preparing future nurses for an increasingly digitized healthcare landscape requires innovation beyond traditional paper-based pedagogies [1]. Despite widespread adoption of electronic health records (EHRs) in clinical practice, many undergraduate nursing programmes continue to use outdated documentation systems in simulation, contributing to a disconnect between classroom learning and clinical realities and preparedness for practice [2,3]. HealthiERSim®, a custom-built simulated EHR platform, was developed in response to this gap. Designed by nurse educators and researchers (authors), it aligns with accreditation requirements and workforce priorities to enhance students’ digital health literacy, documentation skills and confidence in navigating real-world clinical environments [4].
HealthiERSim® was designed and developed at Charles Sturt University in 2023. Nurse educators co-developed the system to ensure alignment with simulation pedagogy and Australian healthcare documentation practices. The platform includes templates for medication charts, care plans, fluid balance charts and dynamic links to real-time clinical guidelines. Launched in 2024, HealthiERSim® was embedded across six Bachelor of Nursing subjects and deployed during both mannequin-based and standardized patient simulations. Built to be pedagogically sound rather than mimic real EHRs, HealthiERSim® scaffolds learning in a controlled, user-friendly interface that gradually increases complexity to match student progress.
All evaluation activities referenced in this manuscript were conducted with approval from the relevant institutional Human Research Ethics Committee. Multiple phases of the HealthiERSim® implementation and review were covered under approved protocols, ensuring adherence to ethical standards in data collection, participant consent and confidentiality.
Evaluation involved feedback from students and educators, along with a sustainability-focused audit on paper usage. Educators reported that student uptake was influenced by how deeply HealthiERSim® was embedded into the subject design. As one educator noted, ‘If paper charts are still in the lab manual, they’ll choose the easiest option. But if HealthiERSim® is the only option, they learn quickly’.
Educators highlighted improved student engagement, digital literacy and more authentic communication with ‘patients’. One reflected, ‘It helped teach not just documentation but also infection control, privacy, and communication, where to place the workstation, how to involve the patient while entering data’.
From a sustainability perspective, early audits showed a reduction in paper chart printing when HealthiERSim® was fully integrated. However, the impact varied across subjects depending on the confidence of individual educators and subject convenors to replace paper-based tools [5]. Plans to transition the platform to the cloud aim to further support sustainable practice by reducing reliance on physical resources and enabling remote access for tutorials and assessments.
Educator feedback suggested HealthiERSim® significantly enhanced teaching by providing a platform that consolidated digital, clinical and interpersonal learning. Students, particularly international cohorts, were enthusiastic: ‘They loved it. They wanted to take selfies with the WOW [workstation on wheels]’, shared one educator. Others noted students’ improved awareness of person-centred care in digital contexts, such as maintaining eye contact and explaining documentation tasks to patients.
Challenges included inconsistent internet access in older buildings and varied educator confidence in using the tool. Yet, even those with minimal digital experience reported that with training and exploration, HealthiERSim® became an accessible and effective resource. Importantly, the system’s design allowed tutors to model digital professionalism and contextualize its importance in clinical practice.
The next phase involves cloud deployment to support 24/7 student access, integration with video-based scenarios and use in formative assessments. Research is underway to evaluate learning analytics, explore the balance between digital documentation and human connection, and investigate how the system supports interdisciplinary learning across allied health and medical programmes.
HealthiERSim® offers a scalable, evidence-informed model for embedding digital health into undergraduate education. It not only supports students in developing digital competence but also fosters sustainable, person-centred care practices. Future studies should examine student outcomes longitudinally, assess the tool’s impact across disciplines and explore opportunities to embed artificial intelligence (AI) for personalized feedback and learning.
None declared.
No external funding was received to support the development or evaluation of this work.
None declared.
None declared.
None declared.
1.
2.
3.
4.
5.
Reyhane Osouli Alamdari 1
ORCID:https://orcid.org/0009-0007-5301-7374
, Mahsa Abdi 1ORCID:https://orcid.org/0009-0002-0597-8684
, Hesam Sakian Mohamadi 1ORCID:https://orcid.org/0000-0001-5016-2911
, Seyed Vahid Mostafavi 1ORCID:https://orcid.org/0009-0003-2688-2945
[1]
emotional awareness,adolescents,serious games,emotional understanding,and non-gendered character
Emotions are a fundamental yet often misunderstood aspect of human experience, particularly during adolescence. Identity-seeking and emotional volatility mark this stage and heighten psychological sensitivity. According to Erikson’s theory, identity formation and self-awareness are central developmental challenges for adolescents, as they attempt to balance internal changes with external expectations [1].
During this period, teenagers face rapid emotional shifts caused by hormonal, psychological and social changes. These fluctuations considerably affect their decision-making, confidence and stress levels, making it difficult for them to regulate emotions effectively. Limited awareness and narrow understanding of these changes can create sensitive vulnerabilities in both personal and social functioning [2].
These challenges require innovative approaches to help adolescents build self-awareness and emotional regulation skills. One promising method is the use of serious games, which combine entertainment with educational objectives to promote learning and psychological growth. Serious games can provide a safe, engaging environment where adolescents explore emotions and practise self-regulation strategies [3].
This article presents the design and application of a serious game developed to enhance emotional self-awareness among adolescents. ‘My Colours game’ integrates psychological principles with interactive storytelling, aiming at helping players to recognize, understand and manage their emotions in realistic scenarios. In examining its potential as an educational tool, this study focuses on the growing field of serious games for mental health and emotional development.
The provided game was developed using Unity™, a cross-platform real-time engine for creating interactive 2D and 3D applications [4]. It is still in the demo stage, and the link is available at the end of the article. It is delivered as a desktop-based serious game, helping adolescents understand and manage emotions through visual psychology and Paul Ekman’s six-emotion classification [5]: anger, sadness, happiness, fear, disgust and surprise (see Figure 1).

The environment of the game’s various emotion shrines and their corresponding emotion-related elements.
Players explore six shrines, each dedicated to one emotion, and must first find three letters narrating personal experiences related to that emotion, illustrating healthy and unhealthy emotional expressions. At each shrine, scenario-based questions require players to choose the most appropriate emotional response. Correct answers restore the corresponding colour to the character, while incorrect answers leave it colourless, indicating incomplete understanding (see Figure 2).

The non-gendered main character partially recoloured after retrieving emotions.
The game allows non-linear progression, enabling players to select which emotions to pursue and in what order, reflecting real-life emotional development. Two endings are possible: recovering four or more colours results in a happy ending with a family reunion, while three or fewer colours lead to a neutral ending where parents remain supportive. Both outcomes emphasize that emotional learning is a personal journey and that failure is acceptable.
The game’s effectiveness was evaluated through a user test with 12 adolescents aged 13–19 (mean age 16–17; 75% female). The goal was to assess the game itself, not to generalize findings to a larger population. Participants played the beta version of the game in a single session and then completed a questionnaire designed by researchers. The survey asked about engagement with inscriptions, letters and scenario-based questions, as well as empathy, emotional reflection and overall experience. We calculated the percentage of participants reporting engagement and emotional impact to analyse the responses.
Results indicated that most participants correctly interpreted happiness, sadness and disgust, while all participants understood colours representing anger and fear. Surprise was the least consistently understood. Participants interacted with inscriptions (91%) and letters (83%), and 75% empathized with the main character. Overall, 66.67% reported a high or very high connection to the story, and 58.33% indicated a powerful impact of the game on their emotional awareness. The character’s lack of gender enhanced personal relatability, though some suggested optional customization in future versions.
These findings suggest that the game successfully facilitated emotional recognition, reflection and empathy among adolescents. ‘My Colours’ combines narrative, symbolic design and psychological theory to create both engaging and educational experiences. The colour-form associations support visual-emotional learning, while scenario-based letters encourage reflection and empathetic thinking. The modular, non-linear design offers multiple endings based on player choices, reflecting the complexity of real-life emotional development.
One challenge encountered during development was selecting distinct colours for emotions that are visually and psychologically appropriate. For example, choosing colours for happiness and surprise required careful consideration to ensure they conveyed the intended emotional responses. Future work can investigate alternative colour choices and visual cues to improve recognition of less consistently understood emotions.
Moreover, new scenarios and optional character customization could expand the game to increase engagement. Further research with larger and diverse adolescent populations is needed to evaluate long-term effects on emotional awareness and self-regulation. Additionally, this innovation could adapt for use in other educational and youth-focused settings, showing the potential of serious games for emotional learning across different contexts.
Reyhane Osouli Alamdari and Mahsa Abdi contributed equally to this work and share equal first authorship. Reyhane Osouli Alamdari: Writing, Research, Game Development, Project Management. Mahsa Abdi: Writing, Research, Game Development. Hesam Sakian Mohamadi: Supervision. Seyed Vahid Mostafavi: Supervision.
The authors received no specific funding for this work.
Not applicable.
This study was conducted as an educational game evaluation with voluntary participation. Informed consent was obtained from all participants and/or their legal guardians. Formal ethics committee approval was not required according to institutional guidelines.
The authors declare that they have no competing interests.
This brief summarizes findings from a combined undergraduate thesis project completed at the University of Art, Tabriz, 2024, developed collaboratively by the team members.
1.
2.
3.
4.
5.
 Incorporating AI conversation agents into simulation-based learning for nursing students
Incorporating AI conversation agents into simulation-based learning for nursing students
 Facebook
Facebook
 Twitter
Twitter
 Linkedin
Linkedin
 Whatsapp
Whatsapp
